

Pick ‘n’ Mix Week 2 February 2023
We are really grateful to Trudie Pestell for sharing this fabulous education initiative that she has been producing for University Hospital Southampton Emergency Department for a while.
Each week we will bring you some clinical pearls to add in to your knowledge and understanding with links to other resources as well as an OSCE of the week. This week has an abdominal theme.
Definition
A zoonotic infection caused by a spirochete of genus Borrelia, a gram negative, anaerobic bacteria, which is transmitted to humans by ixodes ticks. Animals are the primary reservoir, with ticks becoming infected by feeding on an infected animal.
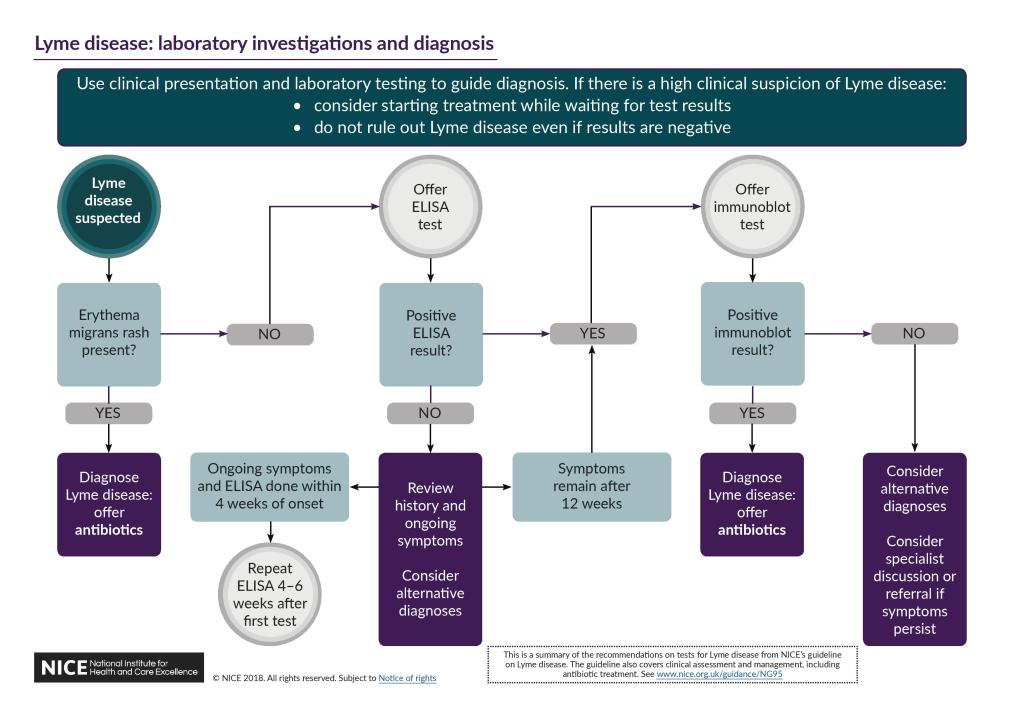
Clinical Features

Erythema migrans is the pathognomnic rash, which usually develops within 1-4 weeks of the bite.
Other features include
- Headache, fever, malaise,
- MSK: arthralgia, arthritis
- CVS: myocarditis,
- Neuro: meningitis, encephalitis, radiculopathy, facial nerve palsy, hearing loss
Risk Factors
- Outdoor activities- recreational, occupational, residential in an area known to have Lyme
- Tick bite duration >= 48 hours
Management
- Over 9yrs: -Doxycycline or amoxicillin for 21 days
- Under 9yrs: -Amoxicillin (21 days) or azithromycin (17 days)
A history of a tick bite AND no symptoms?
Antibiotic prophylaxis is NOT routinely recommended
‘Enjoy the outdoors but be tick aware’
Jarisch-Herxheimer reaction – a side effect of treatment
Potential complication of antimicrobial treatment for any spirochete infection
- Usually occurs in the first 24 hours of treatment
- A cytokine mediated systemic reaction in reponse to dead spirochetes
- Systemic upset: fever, chills, myalgia, headaches
- Self-limiting and usually resolves within 24–48 hours, but it is important to counsel patients on this side effect, as it may mean people discontinue treatment.

The case of traumatic shortness of breath
The beginning:
A 29year old female of no fixed abode presents with shortness of breath & left sided chest pain. She reports that two days previously she was involved in an altercation in which she was stabbed in the left side of the chest. She didn’t initially seek attention as she was afraid of the police becoming involved.
Her observations are:
- Resp Rate – 31/min,
- Oxygen saturations on room air 93% RA,
- Heart Rate 103/minute,
- Blood pressure 111/71.

A chest xray is performed…

The penetrating injury has caused both bleeding and a leak of air into the pleural space.
Use this to practise your abdominal examination. Remember there are resources for lots more system examinations here.
Script
Introduction
” Hello, my name is Phil. I am a medical student .”
“Please can you confirm your name and date of birth, while I wash my hands, put on my PPE and ensure we are somewhere private.”
“Are you comfortable? Do you need any pain relief or a drink?”
“I have been asked to conduct an examination of your knee. This will involve me looking at both knees: how you are walking and assessing the movement and strength. Would that be ok with you?”
“Would you like a chaperone present?”
“I will need to see both your legs, are you able to change into shorts? “
“I will talk out loud as we go”
“If at any time you want me to stop or you are in pain, let me know”
Brief history
- Examiner: my normal practice would be to examine both sides, do you want me to do this?
“Can you briefly tell me what the problem is?”
“What is your occupation?”
“Have you been involved in any trauma?”
“Have you had any previous operations on your knees?”
“Have you been unwell recently?”
Gait
“Please could you walk up and down the room. I am examining for any gait abnormalities, such as…”
- antalgic gait
- Trendelenburg gait
- foot drop
Inspection
“Please can you stand up straight. I am inspecting the hip from the front; back, and sides. I am looking for…”
- scars
- skin changes
- wasting
- muscle bulk of quadraceps
- deformity: varus (out); valgus (in)
- popliteal mass or swelling
Palpation
“Please can you lie down on the couch. I need to feel the knees for…”
Comment on:
- warmth – use the back of your hand to compare to the other side and rest of the leg
- swelling
- bogginess
- crepitus in movement
- pain
“I know need to palpate the joint line or any tenderness, and also assess for effusion”
- Knee flexed at 90o
- Start in the hollow next to medial part of patellar tendon
- Medial joint line → medial tibial plateau (inferiorly) → medial femoral condyle (superiorly) → quads tendon and muscles → lateral femoral condyle → lateral joint line → lateral tibial plateau → patella tendon → fibular head → patella
Effusion
- milk the knee → squeeze thigh and push towards feet
- maintain hold → apply pressure to medial, then later side → looking for a bulge
- Patella tap – larger effusion.
- Empty supra-patellar pouch → push down on patella sharply with thumb and index finger → tap + bounce back if effusion)
Move
Active; passive, resisted (with hand over patella to feel for crepitus)
- flexion
- extension
Special tests
Extensor mechanism
- straight leg raise
Patella apprehension test
- Extended leg, then flex while applying pressure on medial aspect of patella, trying to displace laterally
- Watch patient’s face
Anterior cruciate ligament
- Knees flexed at 90o feet forward
- Sit on patient’s foot
- place thumbs in popliteal fossa with thumbs on tibial tuberosity
- check hamstrings are relaxed
- pull with firm jerk
- positive if there is translocation forward
Posterior cruciate ligament
- Knees flexed at 90o feet forward
- Inspect for sagging of tibial condyle
Medial collateral ligament
- extended legs with knees 20-30o flexed
- one hand on lower leg (this pushes away from side being tested)
- hand outer part of knee, pushing medially, lower hand exerting pressure in opposite direction
- positive if there is joint opening
Lateral collateral ligament
- extended, knees in 20-30o flexed
- one hand on lower leg (this pushes away from side being tested)
- hand inner part of knee, pushing towards lateral side, while lower hand is exerting pressure in opposite direction
- positive if there is joint opening
McMurray’s test – meniscal injury
- Fully flex knee
- MEDIAL:
- Laterally rotate tibia (knee), then extend and flex the knee
- LATERAL:
- Medially rotate tibia (knee), then extend and flex the knee
- Positive if there is popping; cracking; pain
Close
“Thank you Mr X. That is the end of the examination.”
“Do you need any help getting dressed?”
“To complete my examination I would like to…”
- examine the joint above andbelow (hip and ankle)
- PR examination to assess tone and sensation
- examine neurovascular status (if not done)
“My working diagnosis is… I think we should do …”
“Does this sound reasonable to you? Do you have any questions or concerns?”
Infographic






Additional Resources
- Knee examination 1,2
- NICE: How do i exclude fracture using the Ottawa knee rules?
- Knee joint anatomy